Inflammatory Diseases
Conditions in which chronic or dysregulated inflammation is a primary driver of tissue damage and symptoms, distinguishing it from conditions where inflammation is merely an incidental or minor feature.
Research Advances

Boundaries of what qualifies as an “inflammatory disease” continue to shift as research advances — particularly in the fields of neurodegeneration, metabolism, oncology, and psychiatry (where conditions like depression are increasingly being studied for their inflammatory underpinnings).
The list of inflammatory diseases below represents the current medical consensus on diseases where inflammation is a clinically meaningful and generally accepted part of the pathology.
For virtually every disease on that list below, reducing systemic inflammation through lifestyle will produce some measurable benefit — whether in symptoms, disease activity, progression rate, inflammatory biomarkers, or quality of life.
The evidence for this is now substantial across almost every category.
The earlier lifestyle-based inflammation reduction is applied, the greater the proportion of the disease that can be prevented, reversed, or halted.
Proportional Results

Modest, partial lifestyle changes — which is what most clinical trials measure and what most patients implement — produce modest results. But when individuals make comprehensive, sustained, high-compliance changes across diet, exercise, sleep, stress, and gut microbiome health simultaneously, the cumulative anti-inflammatory effect operates through multiple converging biological pathways at once. The gut microbiome restructures, intestinal permeability improves, circulating pro-inflammatory cytokines fall, molecular mimicry triggers are removed, and the dysregulated immune response loses much of its stimulus. This is a fundamentally different biological state than partial intervention achieves, and the clinical outcomes reflect that difference.
The reason this goes under recognised in mainstream studies is largely methodological rather than scientific. Randomised controlled trials cannot easily study high-compliance, multi-modal lifestyle transformation — patients vary too much in what they actually do, and full adherence is difficult to standardise or measure. So the literature systematically underestimates what is biologically achievable, because it measures average compliance in heterogeneous populations rather than what happens at the high end of genuine commitment. The thousands of documented recoveries from inflammatory conditions like RA and AS through lifestyle programs are therefore not anomalies — they are a signal of what the biology actually permits when the inflammatory drivers are addressed comprehensively.
Diagnostic Insight

Additional Conditions
Musculoskeletal symptoms are often the entry point for a huge proportion of inflammatory disease.
Many people with one inflammatory condition have other inflammatory conditions.
Most doctors and specialists essentially run a mental algorithm based on symptom clusters, distribution, timing, and associated features. Which is often not very accurate due to human bias, errors and time laps since training.
Many diseases take years or even decades to get diagnosed on average. Yet understanding the significance of your symptoms early can lead to far better health and well being outcomes.
How this site helps you
You can use the Quiz and the following Assessments – that use questions from the same global diagnostic assessment manuals that doctors and specialists use.
You will receive personalized insights and information. You will be given suggested questions and requests for your health professionals.
After the assessment you will be shown how to take action – to reduce chronic inflammatory drivers and replace them with supportive behaviours that serve your long term health and happiness.
Inflammatory Disease List
Having one inflammatory condition increases your risk of others – 1 in 4 develop a second – so it’s worth reassessing and optimizing your lifestyle for harm minimization and prevention now. You can see below that chronic inflammation can adversely effect just about every part of your body.
Data Organisation
Chronic inflammation plays a significant role in many common conditions. This list organises them by global prevalence and shows the strength of evidence that science driven lifestyle changes can meaningfully reduce inflammatory burden, symptoms, flares, and disease progression.
Tiers:
✅ Strong evidence — Unhealthy Lifestyle is a major driver of disease. Science driven lifestyle changes can be used as a therapeutic tool (backed by guidelines like EULAR and ECCO 2025, meta-analyses, and real-world outcomes).
> Moderate evidence — Lifestyle changes reduce overall inflammatory load and supports better disease outcomes.
MUSCULOSKELETAL & RHEUMATOLOGICAL
Musculoskeletal conditions (especially back pain) are consistently ranked as:
#1 cause of years lived with disability (YLDs) in global burden studies
Many conditions traditionally viewed as “wear and tear” are now understood to have a significant inflammatory component that is highly influence through lifestyle interventions.

✅ Strong evidence — Lifestyle plays a major role in driving or reducing inflammation, symptoms, and progression in the following conditions:
• Osteoarthritis (OA)
(Approx. ~ 10 – 15% of the global population; approx. one billion people.
— Most common arthritis. Increasingly recognised as involving low-grade systemic inflammation driven by obesity, metabolic dysfunction, and diet, in addition to mechanical joint stress.
— Weight loss, exercise, and dietary changes significantly improve pain and function – and there is so much more you can optimize.

• Rheumatoid arthritis (RA)
(Approx. ~0.5–1% global prevalence)
— Chronic autoimmune inflammatory disease.
— Strong evidence that diet, smoking, body weight, and physical activity influence disease activity, flare frequency, and long-term outcomes.

• Chronic low back pain (mechanical–inflammatory overlap)
(Approx. ~7–10% point prevalence globally; lifetime prevalence ~60–70%)
— One of the leading causes of disability worldwide.
— Often involves a combination of mechanical stress, muscle dysfunction, sedentary lifestyle, obesity, and low-grade systemic inflammation.
— Population studies suggest ~30–50% of adults over 50 experience ongoing or recurrent back pain, highlighting a large underdiagnosed burden.
— Lifestyle interventions (movement, strengthening, weight loss, anti-inflammatory diet) significantly improve outcomes.
• Ankylosing spondylitis (AS) / axial spondyloarthritis
(Approx. ~0.1–0.3% global prevalence)
— Inflammatory spinal disease closely linked to gut and immune system activity.
— Lifestyle factors (diet, gut health, exercise, smoking) influence inflammation and disease severity.

• Psoriatic arthritis (PsA)
(Approx. ~0.1–0.3% global prevalence)
— Strong association with obesity and metabolic syndrome.
— Weight loss and dietary changes are shown to reduce disease activity and improve treatment response.
Tendinitis (tendinopathy)
- Affects ~10–20% of adults at any given time (varies by age/activity)
- Extremely common examples:
- Rotator cuff tendinopathy
- Achilles tendinopathy
- Tennis elbow
“tendinopathies, bursitis, enthesitis, and fasciitis also have inflammatory components influenced by lifestyle,”
Plantar fasciitis
- Affects ~4–7% of the population at any given time
- ~10% lifetime risk

Gout (crystal arthritis)
(Approx. ~0.6–1% global prevalence; rising worldwide)
— Inflammatory arthritis driven by uric acid crystal deposition.
— Strongly linked to diet, alcohol intake, obesity, and metabolic syndrome.
— Lifestyle modification plays a major role in reducing flares and disease progression.
Musculoskeletal & Rheumatological - Continued
Moderate evidence — Lifestyle influences overall inflammatory load and disease expression in the following Musculoskeletal & Rhumatological conditions.
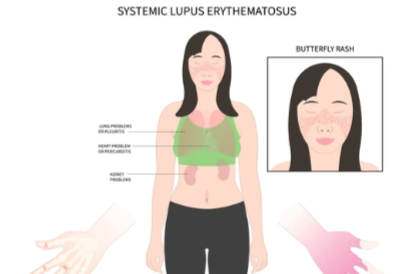
Systemic lupus erythematosus (SLE)
(Approx. ~0.05–0.1% global prevalence)
• Sjögren’s syndrome
(Approx. ~0.05–0.1% global prevalence)
• Systemic sclerosis (scleroderma)
(Approx. ~0.005–0.02% global prevalence)
— Autoimmune connective tissue diseases where lifestyle (diet, stress, physical activity, smoking) influences systemic inflammation, comorbidities, and quality of life, though not primary disease cause.
• Juvenile idiopathic arthritis (JIA)
(Approx. ~0.05–0.1% of children globally)
— Group of inflammatory joint diseases in children.
— Emerging evidence suggests diet, gut health, and lifestyle may influence inflammatory activity, though evidence is less consistent than in adult RA.
• Reactive arthritis, IBD-associated arthritis
— Triggered by infection or associated with gut inflammation; lifestyle influences baseline inflammatory state and recovery.
• Polymyalgia rheumatica (PMR)
(Approx. ~0.1–0.2% in older adults; rare under age 50)
METABOLIC / SYSTEMIC

✅ Strong evidence — Lifestyle directly reverses or dramatically improves these by lowering metaflammation
- Obesity (drives systemic chronic low-grade inflammation)
(Approx. ~15–20% worldwide, higher in developed countries. - Metabolic syndrome
(Approx. ~25–30% of adults worldwide) - Non-alcoholic fatty liver disease (NAFLD / MASLD)
(Approx. ~25–38% of global adult population)
- Non-alcoholic steatohepatitis (NASH / MASH)
(Subgroup of NAFLD with inflammatory progression) - Type 2 diabetes mellitus
(Approx. ~10–11% of global adult population) - Gout (also under crystal arthropathies)
(Approx. ~0.6–1% global prevalence) - Polycystic ovary syndrome (PCOS)
(Approx. ~8–13% of women of reproductive age) - Obstructive sleep apnea (OSA)
(Approx. ~5–10% of adults) — Strong metabolic and inflammatory overlap; weight loss and sleep quality significantly reduce inflammatory burden.
ORAL / PERIODONTAL

✅Strong evidence
Chronic periodontal disease
Severe periodontitis affects ~11% of adults globally, though mild-to-moderate gum disease is extremely common, with estimates up to 50–60% of adults showing some signs.
It is a major source of systemic inflammation and has been strongly linked to the development and progression of cardiovascular disease, type 2 diabetes, and inflammatory arthritis such as rheumatoid arthritis.
Inflammatory impact on rheumatic disease
Periodontal disease can exacerbate joint inflammation and autoimmune responses, increasing disease activity in people with rheumatoid arthritis and potentially contributing to earlier onset or more severe symptoms.
Chronic oral inflammation also contributes to systemic immune activation, which is thought to accelerate vascular inflammation and metabolic disturbances, making it a significant, often under-recognized driver of multimorbidity in adults.
CARDIOVASCULAR
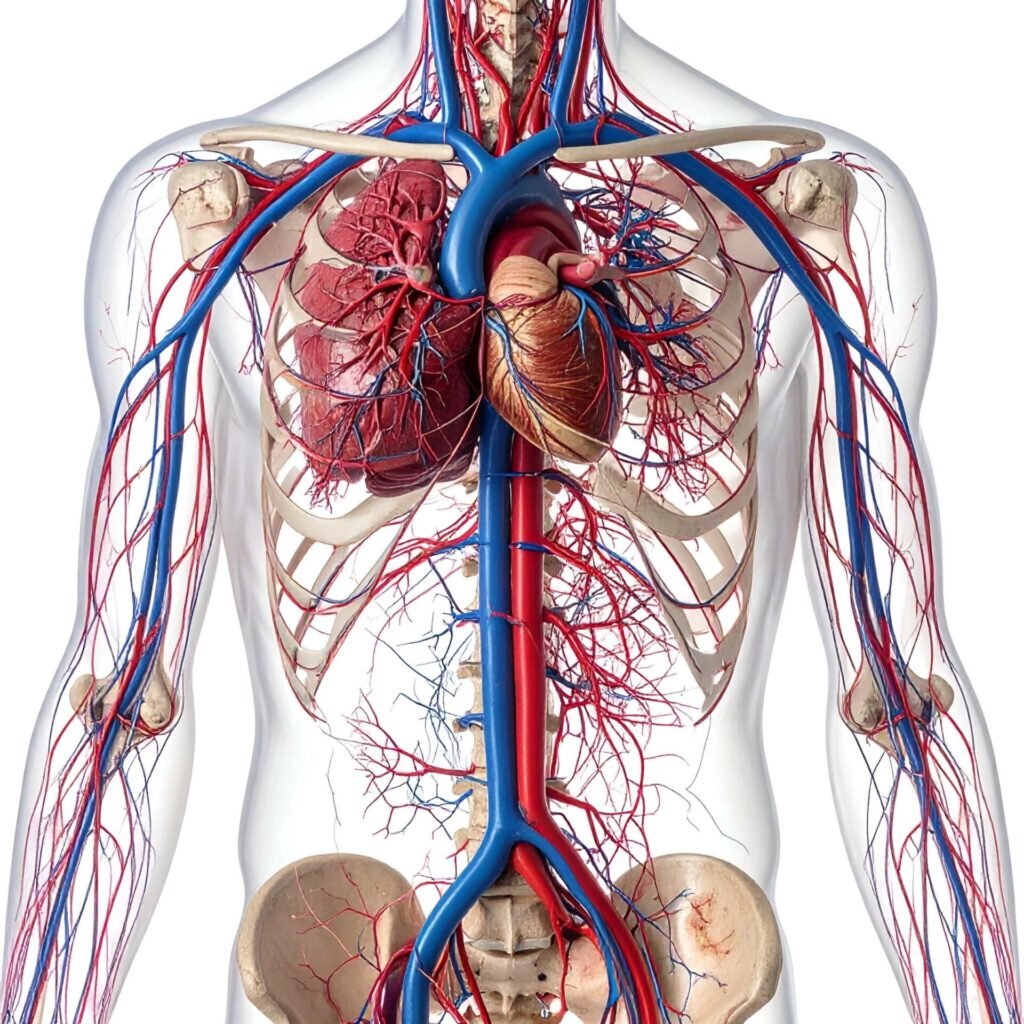
Cardiovascular Disease— Major global burden
✅ Strong evidence — Chronic inflammation (metaflammation) is a core driver of:
• Atherosclerosis / cardiovascular disease
(Approx. ~7–8% diagnosed global prevalence; much higher subclinical burden)
Heart disease is a chronic inflammatory condition, strongly influenced by lifestyle factors.
> Moderate evidence — Lifestyle influences outcomes but is not a primary driver of:
• Myocarditis
• Pericarditis
• Inflammatory cardiomyopathy
(Individually <1% global prevalence; lifestyle influences recovery and baseline inflammation rather than primary disease onset)
GASTROINTESTINAL & HEPATIC

✅ Strong evidence — Lifestyle and diet are key modulators of inflammation
Crohn’s disease
(Approx. 0.2–0.5% of Western populations; rising globally)
Chronic inflammatory bowel disease affecting the GI tract. Lifestyle factors such as diet, obesity, and stress can influence disease activity and outcomes.
Ulcerative colitis (UC)
(Approx. 0.2–0.5% of Western populations)
Chronic inflammation of the colon; strongly influenced by diet, gut microbiome, and systemic inflammation.
Inflammatory bowel disease (IBD)
Umbrella term for Crohn’s disease + UC. Estimated global prevalence: ~0.5% in developed countries. Diet and lifestyle are recognized as important modulators of disease severity.
Coeliac disease (gluten-sensitive enteropathy)
(Approx. 1% globally)
Autoimmune reaction to gluten; lifestyle intervention (strict gluten-free diet) is the primary treatment.
Non-alcoholic steatohepatitis (NASH / metabolic-associated steatohepatitis)
(Approx. 1–3% globally; higher in populations with obesity or type 2 diabetes)
Chronic liver inflammation driven by excess fat accumulation; diet, exercise, and weight management are strongly influential.
Chronic diverticulitis
Subset of diverticular disease with repeated inflammation; diet (high-fiber intake) and lifestyle influence risk. Prevalence in adults >50: ~5–10% for clinically significant cases.
Moderate evidence — Lifestyle may help reduce inflammatory burden
Microscopic colitis (collagenous & lymphocytic colitis)
Rare but diet and lifestyle can modulate symptoms; prevalence ~0.05–0.1%.
Autoimmune hepatitis
(~0.02% globally); some evidence that systemic inflammation influenced by lifestyle may affect disease course.
Primary sclerosing cholangitis (PSC)
(~0.01–0.03%); strongly associated with IBD, systemic inflammation may influence progression.
Primary biliary cholangitis (PBC)
(~0.03–0.05%); rare autoimmune liver disease with some modulation possible through lifestyle.
Eosinophilic gastroenteritis / eosinophilic oesophagitis
Rare, but symptoms can be triggered by diet (food allergens) and inflammation.
IgG4-related disease
Multi-organ inflammatory condition; rare, diet/lifestyle influence unclear but chronic inflammation management is important.
NEUROLOGICAL (Neuroinflammatory)
✅Strong evidence — Lifestyle and inflammation are key modulators
Alzheimer’s disease / dementia
(Approx. 5–7% of people >60 globally)
Chronic low-grade neuroinflammation contributes to neurodegeneration; diet, physical activity, sleep, and cognitive stimulation reduce risk and slow progression.
Multiple sclerosis (MS)
(Approx. 0.03–0.1% globally; higher prevalence in Western countries)
Autoimmune demyelinating disease; evidence supports influence of vitamin D, diet quality, exercise, and smoking cessation on disease activity.
Moderate evidence — Lifestyle may improve inflammatory burden and outcomes
Major depressive disorder / depression
(Approx. 5–6% global prevalence)
Low-grade systemic inflammation is increasingly recognised as a contributor; exercise, anti-inflammatory diets, sleep optimisation, and stress reduction improve outcomes.
Parkinson’s disease
(Approx. 0.1–0.2% globally; increases with age)
Neuroinflammation contributes to disease progression; lifestyle factors such as exercise and diet influence symptom trajectory.
Neuroinflammatory conditions with moderate lifestyle influence
lifestyle can influence symptoms or low-grade neuroinflammation
Autism Spectrum Disorder (ASD)
(Approx. ~1–2% of children globally)
Some evidence suggests neuroinflammation and immune dysregulation in a subset of individuals. Diet and lifestyle interventions (e.g., gluten-free/casein-free or anti-inflammatory diets, sleep, stress management) may improve secondary symptoms and overall health, but are not curative.
Chronic Fatigue Syndrome / Myalgic Encephalomyelitis (CFS/ME)
(Approx. ~0.2–0.4% globally; higher in women)
Low-grade neuroinflammation is increasingly recognised. Anti-inflammatory diets, pacing, sleep optimisation, and stress reduction can improve symptom burden and functional capacity, although no interventions currently reverse the condition.
RESPIRATORY

✅ Strong evidence – that they are environmental and lifestyle driven
• Asthma
(Approx. ~5–10% global prevalence)
• Chronic obstructive pulmonary disease (COPD)
(Approx. ~10–12% of adults over 40 globally)
• Chronic bronchitis
(Approx. ~3–7% global prevalence)
— Strongly linked to smoking, pollution, and chronic inflammatory exposure
>Moderate evidence
• Allergic rhinitis, non-allergic rhinitis, chronic sinusitis
(Approx. ~10–30% globally)
• Sarcoidosis, interstitial lung disease (ILD)
(Low prevalence individually; systemic inflammation influenced by lifestyle factors)
(lifestyle influences recovery and baseline inflammation rather than primary disease onset)
SKIN (Dermatological)

✅ Strong evidence
- Psoriasis
(Approx. ~2–3% global prevalence) - Psoriatic arthritis (PsA)
(Approx. ~0.1–0.3%) diagnosed - Atopic dermatitis (eczema)
(Approx. ~10–20% globally; higher in children) - Hidradenitis suppurativa
(Approx. ~1–4%) - Rosacea
(Approx. ~5% globally)

CANCER (Inflammation-Driven)

Moderate evidence
- Colorectal cancer
(Approx. ~0.5–0.6% prevalence; lifetime risk ~4–5%) - Liver cancer (hepatocellular carcinoma)
(Approx. ~0.1–0.2%) - Gastric cancer
(Approx. ~0.2–0.3%)
— Lifestyle influences inflammatory environment, risk, and progression.
RENAL (Kidney)

✅Strong Evidence
Chronic kidney disease (CKD, inflammatory component)
- Approx. ~10% global prevalence.
- Strongly influenced by diet, obesity, hypertension, metabolic health, and systemic inflammation
Moderate evidence
IgA nephropathy, lupus nephritis
- Rare individually (~0.01–0.05%), autoimmune origin.
- Some evidence that diet and lifestyle can modulate inflammatory activity alongside medical care.
ENDOCRINE

✅Strong Evidence
Type 2 diabetes mellitus (T2DM)
Approx. ~8–10% global prevalence. Chronic low-grade inflammation contributes to insulin resistance. Lifestyle (diet, weight, activity) strongly influences risk and progression.
Hashimoto’s thyroiditis
Most common autoimmune thyroid disease (~5% globally; higher in women). Leads to hypothyroidism. Lifestyle and gut health may help modulate autoimmune activity.
Graves’ disease
Autoimmune hyperthyroidism (~1–2%). Anti-inflammatory lifestyle can support management.
Moderate Evidence
Type 1 diabetes mellitus (T1DM)
Autoimmune beta-cell destruction (~0.1–0.3%). Diet and lifestyle may influence inflammatory activity.
Addison’s disease (autoimmune adrenalitis)
Rare; lifestyle may support immune regulation but is primarily managed medically.
EYE (Ophthalmic)

Moderate Evidence Lifestyle effects:
(For influence from lifestyle factors)
Uveitis (including iritis)
(Approx. ~0.1–0.2% globally)
— Strongly linked to systemic inflammatory diseases (SpA, IBD); lifestyle influences systemic inflammatory load.
Dry eye disease (DED)
(Approx. ~5–30% globally)
— Chronic inflammatory surface disease influenced by diet, environment, and systemic inflammation.
Blepharitis / Meibomian gland dysfunction
(Approx. ~5–10%)
Episcleritis / Scleritis
(Low prevalence but autoimmune association)
EAR

Moderate evidence lifestyle effects:
• Chronic otitis externa
(Chronic outer‑ear inflammation; lifetime prevalence of otitis externa ~10% of people, with a small subset becoming chronic)
— Persistent inflammation of the external ear canal can lead to pain, itching, and canal narrowing. While often initially infectious, chronic cases may be prolonged by local and systemic inflammatory burden.
• Chronic otitis media / chronic suppurative otitis media (CSOM)
(Approx. ~3–4% global prevalence or ~300+ million people worldwide)
— Long‑standing middle ear inflammation and perforation of the eardrum often coexist with hearing loss and, in some cases, vestibular symptoms. CSOM is a significant source of chronic local inflammation and contributes to the overall burden of ear disease.
• Autoimmune inner ear disease (AIED)
(Estimated prevalence ~15 per 100,000 people)
— A rare immune‑mediated inner ear inflammation that can lead to progressive hearing loss and vestibular symptoms. AIED is often associated with systemic autoimmune conditions such as rheumatoid arthritis or vasculitis.
• Relapsing polychondritis (ear involvement)
(Rare; approx. ~4.5 cases per million people)
— Autoimmune inflammation targeting cartilage, including the external ear and other cartilaginous structures. This rare disorder can present with repeated episodes of painful auricular inflammation and is strongly linked with systemic autoimmune disease.
REPRODUCTIVE & UROGENITAL

✅ Strong evidence for:
Endometriosis
(Approx. ~10% of women of reproductive age)
A condition where tissue similar to the uterine lining grows outside the uterus, causing chronic pelvic pain, painful periods, and sometimes infertility. Often associated with low-grade systemic inflammation, which can contribute to wider inflammatory symptoms.
“Endometriosis symptoms often fluctuate with hormonal cycles, but systemic inflammation contributes to chronic pain and fatigue.”
Moderate evidence for:
Chronic prostatitis
(Approx. ~2–10% of men)
Persistent pelvic pain, urinary symptoms, and inflammation of the prostate, often associated with systemic low-grade inflammatory responses.
Interstitial cystitis
(Approx. ~0.5–1%)
A chronic bladder condition causing pelvic pain, urinary urgency, and frequency, with inflammation of the bladder wall contributing to both local and systemic inflammatory effects.