TNF Inhibitors
TNF-alpha blockers can reduce aggressive inflammation fast and protect joints when it matters most. They’re potent tools – but not curative – and come with real risks and costs. Use them wisely while you repair root causes through lifestyle, then consider careful tapering with medical supervision.
Key takeaways
TNF-α fuels many features of inflammatory arthritis; blocking TNF-α rapidly reduces swelling and pain.
TNF inhibitors carry boxed warnings (serious infections, malignancy, cancer) and special cautions (demyelination, heart failure).
Pre-treatment screening (TB, hepatitis), vaccinations, and ongoing labs are essential.
Costs are substantial, though biosimilars and assistance programs can help.
Weight gain can occur in some users – track weight and body composition.
Treat-to-target with possible tapering is feasible for selected patients in remission – discuss with your medical practitioner.
Visceral fat, dysbiosis/LPS, stress, poor sleep, and certain dietary components raise TNF-α.
Omega-3s, curcumin, movement, a careful diet, sleep, and stress reduction lower TNF signaling and symptoms over time.
Botanicals like boswellia, quercetin, and sulforaphane show benefit in early trials; treat as adjuncts.
Coffee’s impact appears individual; pay attention to your own flare patterns.
IBS links to TNF are inconsistent; IBD is clearly TNF-driven.
Use medicines wisely to protect tissue now, and lifestyle to reduce the need for medicines later – with clinician guidance.
TNF-α Blockers & Natural Modulators
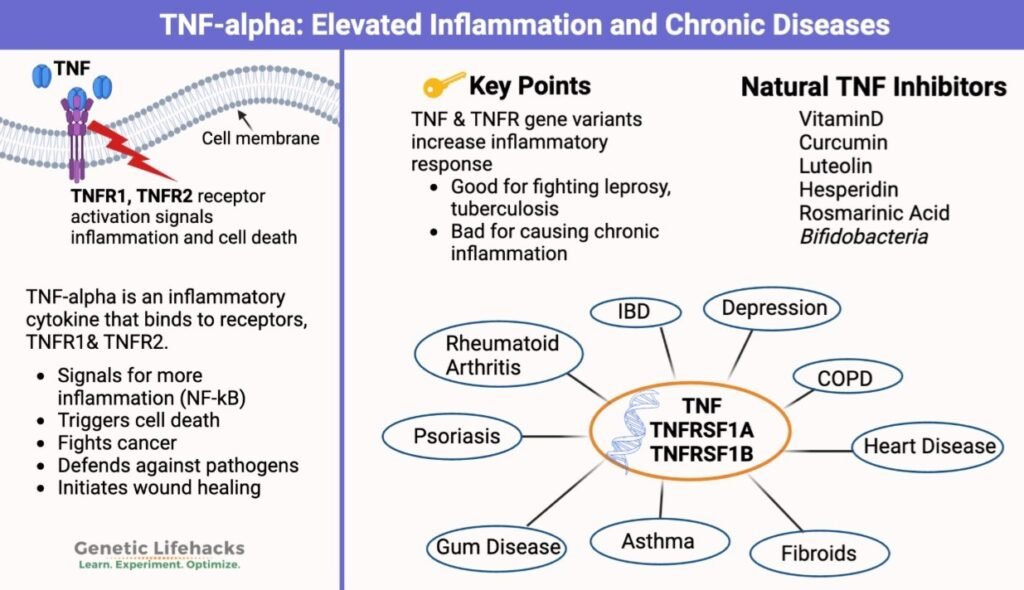
What TNF-α does – and why it matters
Tumor Necrosis Factor-alpha (TNF-α) is a fast-acting immune signal (cytokine) that helps us fight infections and clear damaged cells. When chronically elevated, it drives synovial inflammation, bone erosion, fatigue, and pain in immune-mediated diseases – especially rheumatoid arthritis (RA), psoriatic arthritis (PsA), and axial spondyloarthritis or ankylosing spondylitis (axSpA & A.S.). TNF-α also plays roles in inflammatory bowel disease (IBD); However, evidence for classic irritable bowel syndrome (IBS) is mixed. In arthritis care, blocking TNF-α can rapidly reduce swelling and protect joints – but it does not “cure” the upstream drivers of inflammation and there are significant risks with these drugs.
Part 1 – Prescription TNF-α inhibitors (TNF i)
How the drugs work
Five TNF inhibitors are used widely:
Etanercept (Enbrel®) – a soluble TNF receptor fusion protein (subcutaneous).
Adalimumab (Humira® and biosimilars) – monoclonal antibody (subcutaneous).
Infliximab (Remicade® and biosimilars) – monoclonal antibody (intravenous).
Golimumab (Simponi® or Simponi Aria®) – monoclonal antibody (subcutaneous or intravenous).
Certolizumab pegol (Cimzia®) – PEGylated Fab’ fragment (subcutaneous).
By neutralizing TNF-α, these agents quickly lower synovitis, pain, and acute-phase reactants, and they slow radiographic damage – especially when started early and combined with methotrexate. In RA, roughly 60 to 70% of patients achieve ACR20 responses within 3 to 6 months, and many reach low disease activity or remission under treat-to-target strategies.
Common benefits across conditions
Rapid reduction in joint swelling and morning stiffness (often within weeks).
Lower ESR & CRP and improved function.
Slower radiographic progression when continued at target.
Safety profile (what to know before starting)
Class boxed warnings & major risks (all TNFi):
Serious infections (bacterial, mycobacterial/TB, invasive fungal); screen for TB and hepatitis B before therapy; monitor during/after treatment.
Malignancy: signals for lymphomas (including rare hepatosplenic T-cell lymphoma in specific high-risk IBD settings) and non-melanoma skin cancers.
Demyelinating disease: rare optic neuritis, MS-like syndromes, Guillain-Barré; generally avoid if there is a history of demyelinating disease.
Heart failure: new or worsening CHF reported with some agents; use caution in patients with known HF and involve cardiology as needed.
Other considerations: cytopenias, liver enzyme elevations, paradoxical psoriasis or uveitis, autoantibody formation (e.g., ANA), and injection or infusion reactions. Review vaccinations (including recombinant zoster) prior to or during therapy according to immunization guidance. Avoid live vaccines while immunosuppressed.
Monitoring before & during therapy: Tuberculosis testing, hepatitis B & C risk assessment, complete blood count, liver function tests and regular skin cancer checks. TNF inhibitors suppress part of the immune system, so ongoing vigilance for infections and certain cancers is important.
Drug-by-drug snapshot (benefits • dosing • key risks • indicative cost)
Note on costs: list prices vary by country, strength, and payer. U.S. examples below reflect typical wholesale/list ranges and may be substantially reduced by insurance, biosimilars, patient-assistance programs, and site-of-care arrangements. Always check the current local formulary.
Etanercept (Enbrel®)
Use: RA, PsA, A.S. and axSpA, JIA, plaque psoriasis.
Typical dosing: 50 mg injection weekly (or 25 mg twice weekly).
Notables: fast onset; often combined with methotrexate in RA.
Key risks: serious infections; malignancy; demyelination warnings; heart failure cautions; rare severe hematologic events.
U.S. cost: often in the US$1,500–$2,000 per week range at list, before coverage and programs.
Adalimumab (Humira®; many biosimilars)
Use: RA, PsA, A.S. or axSpA, Crohn’s, UC, uveitis, psoriasis, others.
Typical dosing: 40 mg injection every other week (some weekly).
Notables: broad labels; numerous biosimilars may reduce acquisition cost.
Key risks: serious infections; malignancy warnings (including HSTCL signal in certain high-risk IBD populations); demyelination warnings.
U.S. cost: brand list prices are high; biosimilar adoption and payer contracts can substantially lower patient cost.
Infliximab (Remicade®; biosimilars)
Use: RA (with methotrexate), A.S. oraxSpA, PsA, Crohn’s, UC, psoriasis.
Typical dosing: intravenous at weeks 0, 2, and 6, then every 6–8 weeks; weight-based.
Notables: infusion center administration; premedication sometimes used; immunogenicity reduced by concomitant methotrexate in RA.
Key risks: class warnings; infusion reactions; antibodies if used as monotherapy.
U.S. cost: highly variable; hospital vs ambulatory infusion and biosimilar use can shift totals by thousands per infusion.
Golimumab (Simponi® injection or Simponi Aria® Intravenous)
Use: RA (with methotrexate), PsA, A.S. or axSpA, UC.
Typical dosing: injection monthly; intravenous every 8 weeks after loading.
Key risks & cost: class warnings; costs similar to other TNFi on a monthly basis, payer-dependent.
Certolizumab pegol (Cimzia®)
Use: RA, PsA, AS/axSpA, Crohn’s.
Typical dosing: Injection at weeks 0/2/4, then every 2–4 weeks.
Notables: PEGylated Fab’ fragment without an Fc domain; minimal placental transfer late in pregnancy.
Key risks & cost: class warnings; costs in line with other SC TNFi.
Weight change: several cohorts note modest average weight gain after TNFi initiation; magnitude varies by drug and baseline status. Clinically meaningful gain occurs in a minority but merits monitoring.
Can you taper or space doses once you’re well?
In treat-to-target care, selected patients in stable remission sometimes reduce dose or extend intervals under supervision. Randomized trials show some patients maintain control after dose reduction, but relapse risk rises, and tight monitoring is essential. Taper only after sustained low disease activity or remission and with a shared plan for rapid re-escalation if objective inflammation returns.
Anecdotal studies and case studies show that low or no drug remissions are far more likely if lifestyle changes are made.
Part 2 – Why TNF-α runs high (and what you can change)
TNF-α is elevated by a mix of genes and environment. Common contributors include:
Adiposity & visceral fat: adipose tissue and resident immune cells – produce TNF-α. Weight reduction lowers adipose TNF expression and systemic inflammatory tone.
Microbiome & gut barrier: dysbiosis and endotoxemia (lipopolysaccharide, LPS) activate TNF. Diet triggers, chemicals, emulsifiers and many other factors affect permeability.
Psychological stress: chronic social/psychological stress is linked to higher pro-inflammatory signalling, including TNF, in susceptible individuals.
Sleep disturbance & circadian disruption: fragmented or restricted sleep can increase TNF gene expression; restoring adequate, regular sleep helps normalize immune balance.
Dietary pattern & fatty acid balance: low omega-3 status, ultra-processed foods, excess refined carbs and saturated fats (e.g., palmitate) favor TNF-α signalling; shifting toward omega-3s and whole foods while removing any triggering foods is anti-inflammatory.
Smoking, air pollution, heavy alcohol, and intercurrent infections can all escalate TNF activity via oxidative stress and innate immune activation.
Part 3 – Evidence-based natural ways to lower or modulate TNF-α
Unlike TNF-inhibitor medications, which blunt TNF-α activity across the immune system, lifestyle and dietary approaches tend to normalize TNF-α by reducing the underlying drivers of chronic inflammation, improving metabolic, gut, and immune regulation. These natural methods support immune balance rather than immune suppression and therefore do not appear to carry the same increased risk of infection or cancer when used appropriately.
Important: The items below range from strong clinical evidence to preliminary and experimental. None is a substitute for urgent medical care when joints, eyes, or organs are at risk. Use them to reduce baseline inflammatory drive so medication dependence can often fall over time – with medical supervision.
Lifestyle “big rocks”
Anti-inflammatory, Stick to a whole-food pattern (e.g., plant-forward or oil-free whole-food plant-based when appropriate) with adequate EPA & DHA (food or supplement) and abundant polyphenol-rich plants. Omega-3 supplementation reduces inflammatory cytokines in randomized trials and meta-analyses; typical studied intakes are 1–3 g/day EPA+DHA with meals.
- Oral health – chronic gum inflammation can raise TNF-alpha levels, contributing to increased inflammation throughout the body.
Weight reduction if needed (visceral fat is a TNF source). Even 5–10% weight loss improves inflammatory markers; larger sustained losses yield larger changes.
Regular, moderate exercise (150–300 min/week + 2–3 resistance sessions) lowers baseline inflammation and induces anti-inflammatory myokines; avoid extreme overreaching during flares.
Sleep optimization (7–9 hours, consistent schedule, light/digital hygiene) to reduce stress–inflammation coupling; screen/treat OSA when indicated.
Stress skills (mindfulness, CBT, breathwork, social connection) to quiet neuro-immune activation.
Alcohol and smoking cessation, and air pollution avoidance where possible.
Nutrients & botanicals with human data touching TNF-α (selected)
Omega-3 EPA/DHA: lowers TNF-α/CRP in multiple randomized trials/meta-analyses; supports symptom reduction in inflammatory arthritis.
Curcumin (turmeric extracts, enhanced bioavailability): suppresses NF-κB and downstream TNF-α; meta-analyses show reductions in inflammatory markers and symptom relief in arthritis. Typical trials use 500–1,000 mg/day curcuminoids in enhanced-absorption forms; monitor for anticoagulant interactions.
Boswellia serrata: small RCTs report reductions in pain and stiffness; mechanisms include 5-LOX and cytokine modulation (including TNF).
Quercetin: some RCTs report reductions in CRP/TNF in metabolic/inflammatory contexts; overall effect sizes are modest; possible CYP3A4 interactions.
Sulforaphane (broccoli sprout extracts): activates Nrf2 and dampens NF-κB/TNF signaling in human and translational studies; early clinical data are promising.
Vitamin D (repletion if deficient): immunomodulatory; mixed effects on TNF in trials, but correction of deficiency is standard care.
Probiotics (e.g., selected Bifidobacterium strains): strain- and condition-specific evidence shows TNF reduction in some GI inflammatory contexts.
Additional, emerging, or context-dependent candidates
Evidence here ranges from small human trials to mechanistic, preclinical work and anecdotal evidence.
- Dietary triggers – Anecdotal evidence suggests these are very important to address. Evidence is low because they are so tricky to study.
- β-glucans (yeast & fungi): immunomodulatory; some human studies show improved host defense and lowered inflammatory signals, though effects on TNF vary by product and context.
- Mushrooms – common varieties like button mushrooms contain compounds shown to help reduce TNF-alpha–driven inflammation.
Polyphenols—luteolin, hesperidin, rosmarinic acid: anti-inflammatory in vitro/animal studies; early human data show mixed improvements in inflammatory markers with limited TNF-specific trials.
Boron: Early clinical studies suggest anti-inflammatory effects (CRP/TNF), but data are limited; avoid excess intake.
Coffee/caffeine: observational findings conflict across populations (some report higher TNF, others lower systemic inflammation depending on dose, preparation, genetics). Treat as individualized—reduce or remove if you notice symptom spikes.
Putting it together: a practical plan
Stabilize quickly when needed. If joints or eyes are threatened—or pain and swelling are severe – TNF inhibitors can be the fastest way to protect tissues. Start with clear goals (treat-to-target), up-to-date vaccines, and monitoring.
Build your “inflammation-lowering base.” Nutrition (adequate omega-3s; minimally processed, plant-rich meals), removal of food triggers, movement, sleep, and stress skills are the durable levers that modulate the same immune pathways drugs target. Track CRP/ESR (and sometimes cytokines) plus symptoms to see objective progress.
Plan for de-escalation – safely. After sustained low disease activity and lifestyle changes, discuss dose spacing or tapering with your rheumatologist; success rates vary, and rapid re-application of TNF lowering protocols should be made if disease returns.
Personally
Once functioning well with little pain, I found that keeping the TNF inhibiter at low or non existent levels allowed me to be aware of the changes in my inflammation due to lifestyle and in particularly, diet. I used the very small amounts of morning pain or joint pain as my guide to understand the effects of these various lifestyle changes. Testing and documenting variations of over many years while continuing daily research.
It is possible I have allowed some continued damage to my joints by allowing this slight inflammation to give me feedback in finding my way to natural remission. But I now have Zero pain or stiffness, even when waking and I can run and am more flexible than most people my age. So I don’t believe I have done much damage. My inflammation markers on the low side of the healthy range.
The alternative was high dose TNF Inhibiters and associated risks (like infections and cancer) without ever fully understanding the root causes of inflammatory disease. I would have likely been dependent on synthetic drugs for the rest of my life.
That said, as far as I can see it is statistically more beneficial to take TNF inhibiters than allow a high level of uncontrolled inflammation. So if I did not have the knowledge and will power to stop the drivers of inflammation, or lifestyle changes did not work for me, then I would take the medication.
Disclaimer
This page is informational and not medical advice. Do not start, stop, or change any medication or supplement without guidance from your qualified health professional. See the site’s full disclaimer for details.