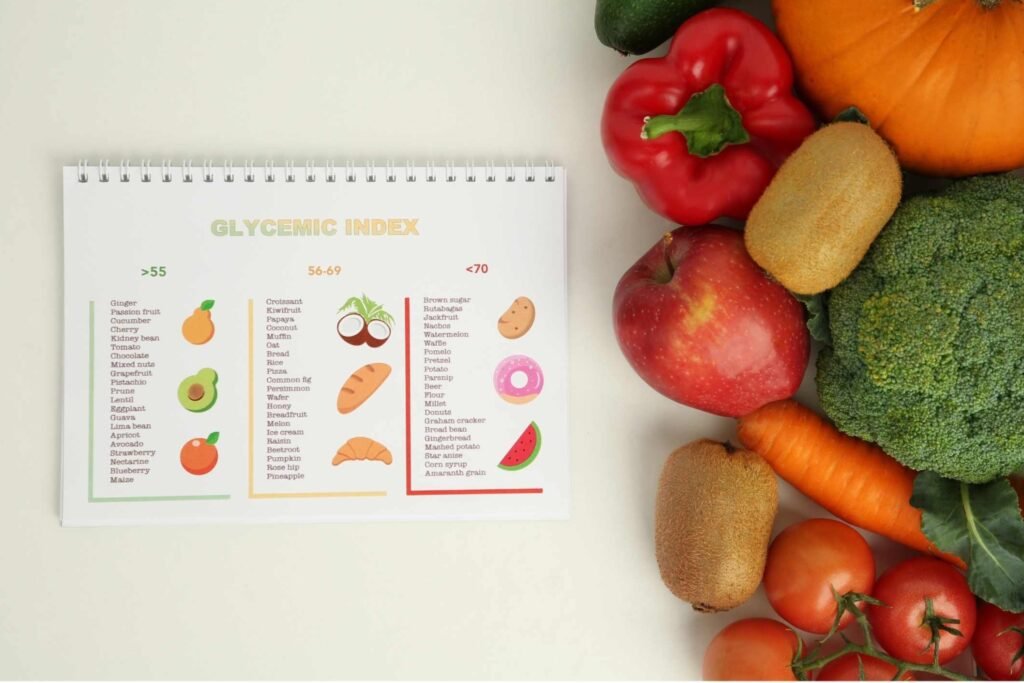
Glycaemic Index
Metabolic Health as an Anti‑Inflammatory Strategy
Chronic inflammation is driven by patterns of metabolic stress. Blood glucose instability, insulin dysregulation, and repeated post‑meal glucose spikes create a persistent inflammatory environment that directly worsens autoimmune disease, inflammatory arthritis, gut inflammation, neuroinflammation, and systemic immune activation.
This page explains:
How blood glucose drives inflammatory signalling
Why patterns matter more than numbers
How food combinations, timing, movement, and eating behaviour shape inflammation
How to eat enough calories while minimising inflammatory load
How this applies to vegan and plant‑based diets
Why fasting reduces inflammation, but chronic under‑eating can increase it
This is not about low‑carb ideology.
Healthy eating is about metabolic stability, immune calm, and physiological resilience.
Glycaemic Control, Blood Sugar Stability & Inflammation
Blood Glucose as an Inflammatory Signal
Glucose in food is fuel, but also a biological signal.
When blood sugar rises, the body does not only see energy availability, it also activates immune, inflammatory, and stress pathways.
Hyperglycaemia means elevated blood glucose levels.
Post-meal hyperglycaemia refers specifically to the rise in blood sugar that occurs after eating, especially after carbohydrate-containing meals.
Human and animal studies consistently show that repeated post-meal hyperglycaemia activates multiple inflammatory and immune pathways, including:
• NF-κB activation
(the body’s master inflammatory control switch that turns on inflammation-related genes) and
• Increased inflammatory markers, including:
– IL-6 (Interleukin-6)
– TNF-α (Tumour Necrosis Factor-alpha)
– CRP (C-reactive protein)
(these are laboratory markers of systemic inflammation)
Post-meal hyperglycaemia also causes,
• Increased oxidative stress
(excess production of reactive oxygen species that damage cells and tissues)
• Endothelial dysfunction
(inflammation and damage to the lining of blood vessels)
• Increased AGE formation (Advanced Glycation End-Products)
(toxic sugar-protein compounds that trigger immune activation and tissue inflammation) and
• Immune cell metabolic switching
(immune cells shift into a high-glucose, pro-inflammatory state that promotes chronic inflammation)
These processes do not automatically cause disease.
However, repeated activation creates a state of chronic low-grade inflammation, which drives long-term tissue damage, immune dysregulation, and degenerative disease.
Key principle:
It is not a single glucose spike that creates disease –
It is frequency, magnitude, and duration.
Transient glucose rises = adaptive physiology.
But,
Chronic instability = inflammatory physiology
Blood Sugar Stability, Brain Function & Mental Wellbeing
Blood sugar stability doesn’t just protect your body, it protects your mind. Stable glucose supports clearer thinking, calmer emotions, better sleep, and better mental health.
Blood Sugar, Brain Function & Mental Wellbeing
Blood glucose is not only a metabolic signal, it is also a neurological and psychological signal. The brain depends almost entirely on glucose for energy, but it functions best when glucose supply is stable, not fluctuating.
Large glucose swings and repeated spikes are associated with impaired brain signalling, mood instability, and stress-chemistry activation, while stable glucose supports cognitive clarity and emotional regulation.
Stable blood sugar is associated with:
- improved concentration and attention
- better memory and learning capacity
- more stable mood
- reduced anxiety symptoms
- reduced depressive symptoms
- improved emotional regulation
- improved stress tolerance
- reduced irritability
- improved sleep quality
- improved overall sense of wellbeing
Blood sugar instability is associated with:
- brain energy fluctuations
- neuroinflammation
- cortisol activation
- sympathetic nervous system dominance
- mood volatility
- anxiety states
- depressive symptoms
- fatigue and brain fog
- poor sleep quality
- impaired cognitive performance
Mechanisms involved include:
- glucose-driven cortisol release
- neuroinflammatory signalling
- insulin resistance in brain tissue
- altered serotonin and dopamine signalling
- mitochondrial dysfunction in neurons
- oxidative stress in neural tissue
- disrupted circadian rhythm regulation
Simple principle:
Stable glucose = stable brain chemistry
Unstable glucose = unstable neurochemistry
Blood sugar regulation therefore supports not only physical health, but also:
- mental clarity
- emotional resilience
- psychological stability
- stress regulation
- long-term cognitive health
- quality of life
Thresholds & Physiological Zones
There is no single “danger line,” but inflammatory signalling increases progressively as glucose rises:
< 6.0 mmol/L — minimal inflammatory signalling
6.0 – 7.8 mmol/L — normal post-meal physiology if brief
> 7.8 mmol/L — oxidative stress and endothelial activation begin
> 8.5 – 9.0 mmol/L — clear inflammatory pathway activation
Healthy metabolism is not defined by avoiding all glucose rises.
It is defined by:
• fast recovery.
• low variability.
• stable baseline.
• short peaks.
• efficient clearance.
The Multi-Dimensional Nature of Eating
Inflammation is shaped by far more than what food you eat.
It is also shaped by how food is combined, how much is eaten, when it is eaten, how fast it is eaten, and what the body is doing before and after meals.
1, Food Combination (Macronutrient Architecture)
How foods are combined determines digestion speed and glucose response:
- Carbohydrates + fibre leads to slower absorption
- Carbohydrates + protein leads to blunted glucose peaks
- Carbohydrates + fats leads to slower gastric emptying
- Isolated carbohydrates leads to fast spikes
- Liquid carbohydrates leads to fastest spikes
Vegan protein stabilisers:
Lentils
Chickpeas
Black beans
Mung beans
Lupins
Buckwheat
Quinoa
Hemp seeds
Chia seeds
Flax
Pumpkin seeds
These foods provide protein, fibre, minerals, and glucose-buffering effects without inflammatory animal proteins.
2, Portion Size (Glycaemic Load)
Even whole foods become inflammatory at excessive doses.
Inflammation is driven by glycaemic load, not just glycaemic index.
Large carbohydrate loads overwhelm glucose clearance mechanisms even when the foods themselves are healthy.
So avoid overeating – stop at 80% full.
3, Meal Order (Food Sequencing Effect)
Human trials show that eating order significantly alters glucose response.
Optimal sequence:
Fibre – protein – fat – carbohydrates
This sequence:
- slows absorption
- reduces insulin spikes
- reduces glucose peaks
- improves satiety
- lowers inflammatory signalling
4, Eating Speed
Fast eating causes:
- larger glucose peaks
- larger insulin spikes
- poor satiety signalling
- increased overeating
- sympathetic nervous system dominance
Slow eating promotes:
GLP-1 activation
improved insulin signalling
lower glucose peaks
better digestion
parasympathetic dominance
Chewing is a metabolic signal, not just digestion.
5, Circadian Timing
Insulin sensitivity follows circadian rhythm:
Best glucose handling is in the morning and midday
Worst glucose handling is in the late evening and night
Large evening meals increase:
nocturnal glucose
cortisol
inflammation
sleep disruption
6, Movement Timing
Light movement after meals:
increases GLUT4 glucose uptake
clears glucose without insulin
reduces post-meal spikes
lowers inflammatory signalling
Even 10–15 minutes of walking is effective.
7, Exercise as a Glucose Buffer
Muscle is the body’s largest glucose sink.
Resistance training:
increases insulin sensitivity
increases glucose storage capacity
reduces inflammatory load
improves metabolic resilience
8, Stress & Sleep
Stress hormones raise blood glucose independently of food.
A calm nervous system improves glucose handling.
A stressed nervous system worsens glucose handling.
Stress increases cortisol, adrenaline, and noradrenaline.
These hormones:
- signal the liver to release stored glucose (glycogen to glucose)
- reduce insulin sensitivity in tissues
- slow gastric emptying unpredictably
- impair insulin’s ability to move glucose into cells
Result of high stress: higher and longer-lasting blood glucose spikes
Stressed eater:
- higher peak glucose spike
- longer time to return to baseline
- more insulin required
- more inflammatory signalling
- greater oxidative stress
- more fatigue/crash afterwards
Calm eater:
- lower peak
- smoother curve
- better insulin efficiency
- less inflammatory load
- more stable energy
- better satiety signalling
Poor sleep:
increases insulin resistance
raises cortisol
increases inflammation
worsens glucose variability
9, Microbiome
Stable glucose supports:
gut barrier integrity
SCFA production
immune regulation
reduced endotoxin translocation
Anti-Inflammatory Eating Architecture
The goal is glucose harmony.
Structural principles:
stable baseline
small peaks
fast recovery
low variability
adequate calories
high satiety
low inflammatory signalling
Low-Inflammation Vegan Day
Click to View Vegan Meal Plan
This model provides sufficient calories while minimising glycaemic and inflammatory load.
Morning- Water
- Light movement
- Sunlight exposure
- Green tea or herbal tea
Structure: Fibre base → protein → fats → carbs
Example:
- Steamed greens or salad
- Lentils or mung beans
- 1 tbsp Tahini or olive oil
- Buckwheat or oats
- Chia, flax & hemp seeds
- Berries (e.g., organic blueberries)
- 15–20 min walking
- Large vegetable base
- Legumes (black beans, chickpeas, lentils)
- Seeds & nuts
- Olive oil, lemon, mustard seed & ACV dressing
- Moderate starch (sweet potato, quinoa, brown rice, buckwheat)
- Movement & resistance exercise
- Vegetables
- Legumes (optionally fatty fish or egg if tolerated and not vegan)
- A little starch (sweet potato, quinoa, brown rice, buckwheat)
- No late carbohydrate loading
- Parasympathetic activation
- Good sleep hygiene
Fasting verses Under-Eating
Why fasting reduces inflammation:
Fasting is:
structured
time-limited
hormetically adaptive
ketogenic
autophagy-activating
immune-resetting
insulin-lowering
inflammatory-pathway suppressing
It shifts physiology into a repair state.
Why chronic under-eating can be inflammatory:
Chronic calorie restriction without fasting structure causes:
persistent cortisol elevation
HPA-axis activation
thyroid suppression
sympathetic dominance
immune dysregulation
muscle loss
micronutrient deficiency
increased inflammatory signalling
This is a stress physiology, not a repair physiology.
The difference:
Fasting physiology:
temporary
controlled
adaptive
anti-inflammatory
repair-oriented
Chronic under-eating physiology:
persistent
stress-driven
catabolic
pro-inflammatory
degenerative
Simple model:
Fasting = intentional biological reset
Under-eating = chronic biological stress
They activate completely different hormonal and immune pathways.
Core Principles Summary
Anti-inflammatory eating includes regulation of blood sugars
Combine foods intelligently
Eat slowly
Eat fibre first
Move after meals
Eat larger meals earlier
Exercise regularly
Maintain adequate calories
Stabilise glucose
Protect sleep
Reduce stress
Support the microbiome *
References – Glycaemic Control, Blood Glucose & Inflammation
1. Blood Glucose, Inflammation & Oxidative Stress
- Ceriello, A. (2005). Postprandial hyperglycemia and diabetes complications: is it time to treat? Diabetes, 54(1), 1–7. https://doi.org/10.2337/diabetes.54.1.1
- Esposito, K., et al. (2002). Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans. Circulation, 106(16), 2067–2072. https://doi.org/10.1161/01.CIR.0000034509.14906.AE
- Monnier, L., et al. (2006). Activation of oxidative stress by acute glucose fluctuations compared with sustained chronic hyperglycemia in patients with type 2 diabetes. Diabetes Care, 29(3), 455–460. https://doi.org/10.2337/diacare.29.03.06.dc05-1612
- Brownlee, M. (2001). Biochemistry and molecular cell biology of diabetic complications. Nature, 414(6865), 813–820. https://doi.org/10.1038/414813a
2. Metabolic Inflammation & Immune Activation
- Hotamisligil, G. S. (2006). Inflammation and metabolic disorders. Nature, 444(7121), 860–867. https://doi.org/10.1038/nature05485
- Donath, M. Y., & Shoelson, S. E. (2011). Type 2 diabetes as an inflammatory disease. Nature Reviews Immunology, 11(2), 98–107. https://doi.org/10.1038/nri2925
- Saltiel, A. R., & Olefsky, J. M. (2017). Inflammatory mechanisms linking obesity and metabolic disease. Journal of Clinical Investigation, 127(1), 1–4. https://doi.org/10.1172/JCI92035
3. Glucose Variability & Vascular Inflammation
- Quagliaro, L., et al. (2003). Intermittent high glucose enhances apoptosis related to oxidative stress in human umbilical vein endothelial cells. Diabetes, 52(11), 2795–2804. https://doi.org/10.2337/diabetes.52.11.2795
- Monnier, L., Colette, C. (2008). Glycemic variability: should we and can we prevent it? Diabetes Care, 31(Suppl 2), S150–S154. https://doi.org/10.2337/dc08-s241
- Hirsch, I. B., & Brownlee, M. (2010). Should minimal blood glucose variability become the gold standard of glycemic control? Journal of Diabetes and Its Complications, 19(3), 178–181. https://doi.org/10.1016/j.jdiacomp.2004.10.001
4. Fasting, Metabolic Switching & Inflammation Control
- Longo, V. D., & Mattson, M. P. (2014). Fasting: molecular mechanisms and clinical applications. Cell Metabolism, 19(2), 181–192. https://doi.org/10.1016/j.cmet.2013.12.008
- Cheng, C. W., et al. (2014). Prolonged fasting reduces IGF-1/PKA to promote hematopoietic stem-cell regeneration. Cell Stem Cell, 14(6), 810–823. https://doi.org/10.1016/j.stem.2014.04.014
- Patterson, R. E., et al. (2017). Intermittent fasting and human metabolic health. Annual Review of Nutrition, 37, 371–393. https://doi.org/10.1146/annurev-nutr-071816-064634
- Wilhelmi de Toledo, F., et al. (2019). Fasting therapy – an expert panel update of the 2002 consensus guidelines. BMJ Nutrition, Prevention & Health, 2(2), 121–129. https://doi.org/10.1136/bmjnph-2019-000016
5. Plant-Based Diets, Glycaemic Stability & Inflammation
- Barnard, N. D., et al. (2022). A low-fat vegan diet improves glycemic control and cardiovascular risk factors. Nutrients, 14(14), 2926. https://doi.org/10.3390/nu14142926
- Jenkins, D. J. A., et al. (2002). Glycemic index: overview of implications in health and disease. American Journal of Clinical Nutrition, 76(1), 266S–273S. https://doi.org/10.1093/ajcn/76.1.266S
- Slavin, J. L. (2013). Dietary fiber and body weight. Nutrition, 21(3), 411–418. https://doi.org/10.1016/j.nut.2004.08.018
6. Glycaemic Control, Mental Health & Cognitive Function
- Craft, S., & Watson, G. S. (2004). Insulin and neurodegenerative disease: shared and specific mechanisms. The Lancet Neurology, 3(3), 169–178. https://doi.org/10.1016/S1474-4422(04)00681-7
- McIntyre, R. S., et al. (2013). Insulin resistance and depression: pathophysiological mechanisms and treatment implications. Neuroscience & Biobehavioral Reviews, 37(10), 289–302. https://doi.org/10.1016/j.neubiorev.2012.11.005
- Kivimäki, M., et al. (2009). Association between insulin resistance and depression: the Whitehall II study. Psychosomatic Medicine, 71(2), 152–158. https://doi.org/10.1097/PSY.0b013e318190cc88
- Akbaraly, T. N., et al. (2009). Dietary patterns and depressive symptoms in middle age. British Journal of Psychiatry, 195(5), 408–413. https://doi.org/10.1192/bjp.bp.108.058925
- Gómez-Pinilla, F. (2008). Brain foods: the effects of nutrients on brain function. Nature Reviews Neuroscience, 9(7), 568–578. https://doi.org/10.1038/nrn2421
- Strachan, M. W. J., Deary, I. J., & Ewing, F. M. E. (1997). Is type II diabetes associated with an increased risk of cognitive dysfunction? Diabetes Care, 20(3), 438–445. https://doi.org/10.2337/diacare.20.3.438
- Arnold, S. E., et al. (2018). Brain insulin resistance in type 2 diabetes and Alzheimer disease. Nature Reviews Neurology, 14(3), 168–181. https://doi.org/10.1038/nrneurol.2017.185
- Reynolds, A., et al. (2019). Carbohydrate quality and human health: a series of systematic reviews and meta-analyses. The Lancet, 393(10170), 434–445. https://doi.org/10.1016/S0140-6736(18)31809-9
- Jacka, F. N., et al. (2010). Association of Western and traditional diets with depression and anxiety in women. American Journal of Psychiatry, 167(3), 305–311. https://doi.org/10.1176/appi.ajp.2009.09060881
- Thayer, J. F., et al. (2012). A meta-analysis of heart rate variability and neuroimaging studies: implications for stress and health. Neuroscience & Biobehavioral Reviews, 36(2), 747–756. https://doi.org/10.1016/j.neubiorev.2011.11.009